The carpal tunnel is a canal on the palm side of the wrist/hand formed by bony floor and transverse carpal ligament (roof). Within the canal is the medial nerve and nine tendons.
Median nerve entrapment at the carpal tunnel leading to carpal tunnel syndrome is the most common nerve entrapment syndrome in humans with an incidence of 3.5-6.2%.
The diagnosis of carpal tunnel syndrome is primarily clinical, with most patients complaining of numbness and tingling in the thumb, index, and ring fingers of the hand with or without weakness. Electro diagnostic testing may be obtained to assess the severity of injury to the median nerve and differentiate from other common diagnoses such as a multiple nerve issue (peripheral neuropathy) or a nerve pinched in the neck (cervical radiculopathy).
Recent studies have increasingly shown the use of ultrasound as effective to evaluate and manage patients with peripheral nerve entrapment. Diagnostic ultrasound has been shown to be as accurate as EMG/NCS with the diagnosis of carpal tunnel syndrome. Furthermore, the dynamic nature of ultrasound allows the provider to identify impingement that is related to motion, that may otherwise go missed on imaging or nerve testing (Fig. 1).
Ultrasound guided carpal tunnel release with the KEMIS device. The primary goal of any carpal tunnel release is to cut the transverse carpal ligament while avoiding injury to other neurovascular structures, to provide relief to the pinched median nerve. Although it has been reported that endoscopic release may promote a faster recovery compared to the mini-open release, there has been raising concerns regarding increased complications due to the inability to visualize surrounding at-risk structures during the procedure. Ultrasound guided carpal tunnel release combines a single incision with direct ultrasound visualization of at-risk structures.
The KEMIS device is a minimally invasive, single use, disposable that allows the user to take advantage of the benefits of ultrasound guidance, while establishing and maintaining a safe treatment area. The device is inserted through a single <3 mm distal forearm skin incision and into the carpal tunnel, with the use of ultrasound-guidance.
What is the recovery like?
Typically, patients will leave with a small incision on the distal forearm. Most patients will resume usual activities within 3-7 days. Few patients have reported palm pain (Pilar pain) up to 21 days. Initial studies on this device have shown promising results, with faster recovery, less use of pain medication, and faster return to normal function with no reported neurovascular injuries to date.
What are the risks/complications?
As with any invasive procedure, there is always an extremely low risk of infection, that the procedure will not work or not provide relief, or that there is neurovascular injury. The use of ultrasound for pre-procedure screening as well as for guidance during the procedure theoretically reduces these risks.
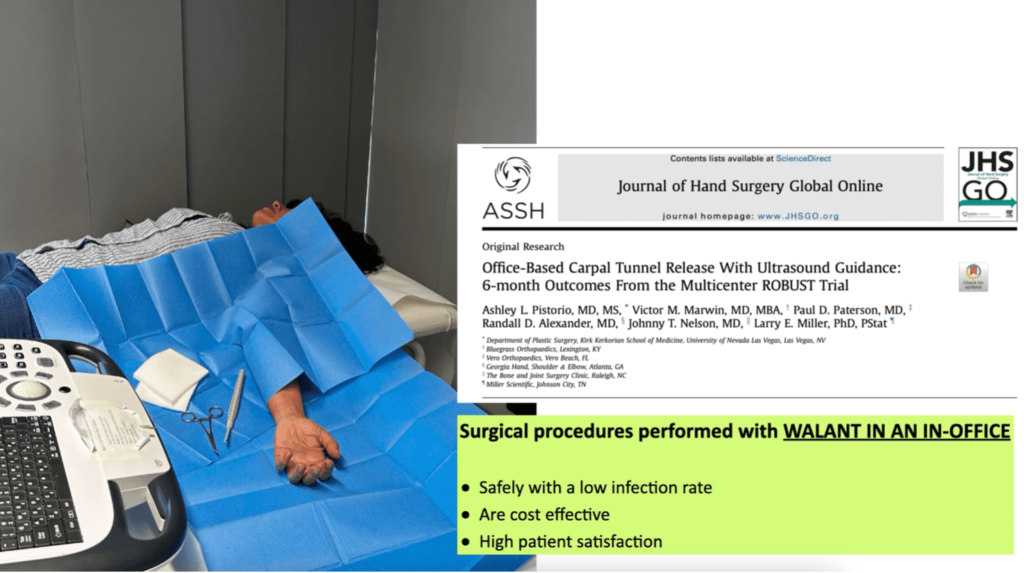
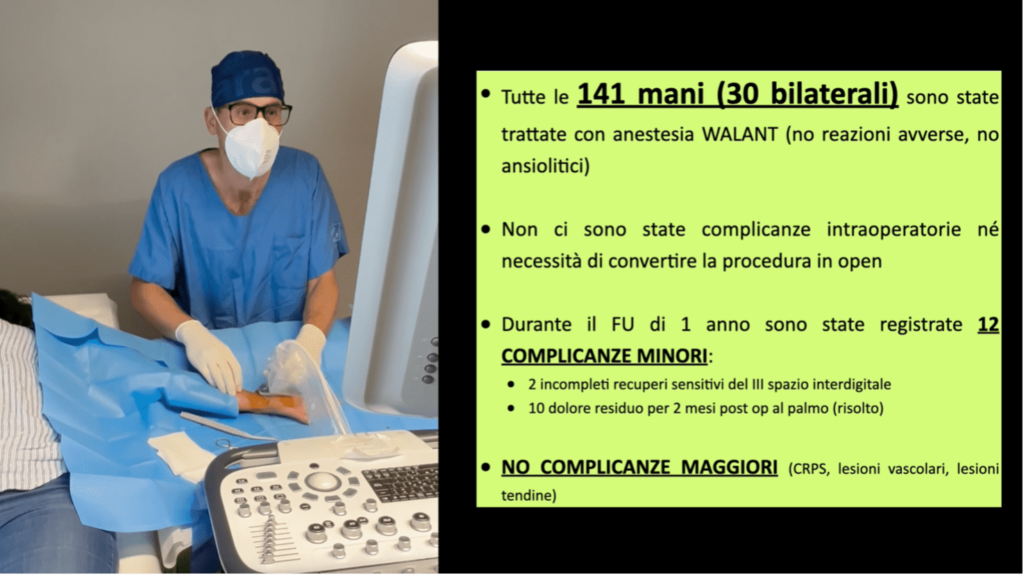
Despite many different devices being used to perform USGCTR, current publications on USGCTR report >98% clinical success rate without any documented neurovascular injuries. Cadaveric investigation using the same device to perform USCTR on cadaveric specimens documented a 100% rate of TCL release and no neurovascular injury. To date over 140 ultrasound-guided carpal tunnel releases have been performed with the KEMIS device without any reported neurovascular complications (Fig. 2).
References
- Poggetti A. 13 EFSM Nanosurfaces scaffold and magnetic nanoparticles to direct the neuronal growth process. future strategies for peripheral nerve regeneration. Antalya, Turkey 21-24 April 2016
- Pourcho AM, Smith J, Henning TP. US-guided carpal tunnel release- Atlas of Interventional Orthopedic Procedures- Book chapter to be published in 2020-2021 in press
- Presazzi A, Bortolotto C, Zacchino M, Madonia L, Draghi F. Carpal tunnel: Normal anatomy, anatomical variants and ultrasound technique. J Ultrasound. 2011;14(1):40-46.
Cartwright MS, Hobson-Webb LD, Boon AJ, et al. Evidence-based guideline: neuromuscular ultrasound for the diagnosis of carpal tunnel syndrome. Muscle Nerve. 2012;46(2):287-293. - Senik RA, Abicalaf CA, Pimentel BF, Braga-Baiak A, Braga L, Cerri GG. Ultrasound features of carpal tunnel syndrome: a prospective case-control study. Skeletal Radiol. 2008;37(1):49-53.
- Abicalaf CA, de Barros N, Sernik RA, et al. Ultrasound evaluation of patients with carpal tunnel syndrome before and after endoscopic release of the transverse carpal ligament. Clin Radiol. 2007;62(9):891-894; discussion 895-896.
- Fowler JR, Cipolli W, Hanson T. A Comparison of Three Diagnostic Tests for Carpal Tunnel Syndrome Using Latent Class Analysis. J Bone Joint Surg Am. 2015;97(23):1958-1961.
Al-Hashel JY, Rashad HM, Nouh MR, et al. Sonography in carpal tunnel syndrome with normal nerve conduction studies. Muscle Nerve. 2015;51(4):592-597. - Ricci V, Becciolini M, Ozcakar L. Ultrasound-Guided Hydrodissection of the Median Nerve in Pronator Syndrome: Where Is the “Pronator Tunnel”? J Ultrasound Med. 2020.
- Watanabe K, Tokumine J, Lefor AK, Moriyama K, Yorozu T. Ultrasound-Guided Hydrodissection of an Entrapped Saphenous Nerve After Lower Extremity Varicose Vein Stripping: A Case Report. A A Pract. 2020;14(1):28-30.
- Poggetti A. 14th IFSSH & 11th IFSHT Triennial Congress with Combined FESSH Congress. How to improve and direct the neuronal growth process. The future for peripheral nerve regeneration. (e-poster) Berlin, Germany, from 17 – 21 June 2019.
- A Poggetti, S Artiaco, B Panero, P Titolo, S Geuna, P Tos. Muscle-Vein-Combined-Graft (Mvcg) for Primary Repair of Crush Nerve Injuries. Riv. Chir. Mano, 49, 2, 279, 2012.
- Stoddard JM, Taylor CR, O’Connor FG. Ulnar Nerve Entrapment at the Cubital Tunnel Successfully Treated with Ultrasound-Guided Peripheral Nerve Hydrodissection: A Case Report and Further Evidence for a Developing Treatment Option. Curr Sports Med Rep. 2019;18(11):382-386.
- Alsaeid MA. Dexamethasone versus Hyaluronidase as an Adjuvant to Local Anesthetics in the Ultrasound-guided Hydrodissection of the Median Nerve for the Treatment of Carpal Tunnel Syndrome Patients. Anesth Essays Res. 2019;13(3):417-422.
- Guo K, McCool L, Wang H, Guo D, Guo D. The Modified Ultrasound-Guided Distal-to-Proximal Carpal Tunnel Injection With Median Nerve Hydrodissection: A Retrospective Safety Review of 827 Procedures. Hand (N Y). 2019:1558944719861715.
- Burke CJ, Walter WR, Adler RS. Targeted Ultrasound-Guided Perineural Hydrodissection of the Sciatic Nerve for the Treatment of Piriformis Syndrome. Ultrasound Q. 2019;35(2):125-129.
- Cass SP. Ultrasound-Guided Nerve Hydrodissection: What is it? A Review of the Literature. Curr Sports Med Rep. 2016;15(1):20-22.
- B. Battiston, P. Tos, A. Poggetti. 11th Congress of European Federation of Societies for Microsurgery. Instructional Course Lecture Neurotization of the brachial plexus: Triceps to axillary nerve. Books of Abstract. Paris April 5th-7th 2012
- Adler AC, Smith DI, Parikh PM. Chronic pain localized to the iliohypogastric nerve: treatment using an ultrasound-guided technique of hydrodissection for catheter placement as a guide for surgical iliohypogastric nerve resection. Plast Reconstr Surg. 2014;134(1):182e-183e.
- Dufour E, Donat N, Jaziri S, et al. Ultrasound-guided perineural circumferential median nerve block with and without prior dextrose 5% hydrodissection: a prospective randomized double-blinded noninferiority trial. Anesth Analg. 2012;115(3):728-733.
- Evers S, Thoreson AR, Smith J, Zhao C, Geske JR, Amadio PC. Ultrasound-guided hydrodissection decreases gliding resistance of the median nerve within the carpal tunnel. Muscle Nerve. 2018;57(1):25-32.
- Poggetti A, Nucci AM, Baluganti A, Pfanner S. Jammed ulnar nerve after distal radius fracture: A case report. JPRAS Open. 2020 Mar 18; 24:20-24. doi: 10.1016/j.jpra.2020.02.005.
- Nordstrom DL, DeStefano F, Vierkant RA, Layde PM. Incidence of diagnosed carpal tunnel syndrome in a general population. Epidemiology. 1998;9(3):342-345.
- Atroshi I, Englund M, Turkiewicz A, Tagil M, Petersson IF. Incidence of physician-diagnosed carpal tunnel syndrome in the general population. Arch Intern Med. 2011;171(10):943-944.
- Palmer DH, Hanrahan LP. Social and economic costs of carpal tunnel surgery. Instr Course Lect. 1995; 44:167-172.
- Keith MW, Masear V, Chung KC, et al. American Academy of Orthopaedic Surgeons Clinical Practice Guideline on diagnosis of carpal tunnel syndrome. J Bone Joint Surg Am. 2009;91(10):2478-2479.
- Fajardo M, Kim SH, Szabo RM. Incidence of carpal tunnel release: trends and implications within the United States ambulatory care setting. J Hand Surg Am. 2012;37(8):1599-1605.
- Poggetti A. SIM Monography. Diagnosi e Trattamento delle Lesioni Traumatiche dei Nervi Perriferici, Chapters related in “Traumatic ulnar nerve lesions”. Pp 59-69. Verduci Editore 2020.